



Annular Elastolytic Giant Cell Granuloma (AEGCG) is a rare granulomatous dermatosis with unclear etiology and physiopathology. Histopathological hallmarks are elastolysis and elastophagocytosis. The definitive mechanism that leads to damage of the elastic fibers has not yet been elucidated. Treatment is still challenging and the use of tetracyclines is controversial due to their potential phototoxicity. Herein, we present a case of generalized AEGCG that achieved a complete resolution after daily doxycycline and review the previous cases treated with tetracyclines.
An 88-year-old man with mild hypertension under treatment with lisinopril, visited our dermatology department presenting multiple erythematous and mild pruritic annular plaques with atrophic center located on the back, shoulders, posterior neck, and upper chest that had appeared over the last month (Fig. 1A). Initial differential diagnosis included subacute cutaneous lupus erythematosus, generalized granuloma annulare and annular psoriasis. A punch biopsy taken from an erythematous border showed a scattered dermal granulomatous infiltrate of multinucleated giant cells with elastophagocytosis consistent with the diagnosis of AEGCG (Fig. 2). Laboratory studies including complete blood cell count, glucose levels, liver and renal function, and antinuclear antibodies were normal. Considering that the lesions were not photo-distributed, the little sun exposure by the patient, and the previously reported cases of AEGCG treated with tetracyclines, doxycycline 100 mg daily was initiated. After five months, complete resolution of the lesions and pruritus were observed (Fig. 1B). Nevertheless, the lesions rapidly recurred when doxycycline was discontinued but after its reintroduction, the patient experienced marked improvement during the following 12 months.
 Multiple erythematous annular plaques on the back and posterior neck at the initial visit. (B) Complete resolution of the lesions after 5 months under treatment with doxycycline 100 mg/day")
 Skin biopsy specimen showing a scattered dermal granulomatous infiltrate with phagocytosis of elastic fibers by multinucleated giant cells. (Hematoxylin & eosin, ×100). (B Elastophagocytosis by multinucleated giant cells demonstrated by elastic fibers stain. The blue arrow indicates the elastophagocytosis. (Verhoeff-Van Gieson; ×100)")
(A) Skin biopsy specimen showing a scattered dermal granulomatous infiltrate with phagocytosis of elastic fibers by multinucleated giant cells. (Hematoxylin & eosin, ×100). (B Elastophagocytosis by multinucleated giant cells demonstrated by elastic fibers stain. The blue arrow indicates the elastophagocytosis. (Verhoeff-Van Gieson; ×100)
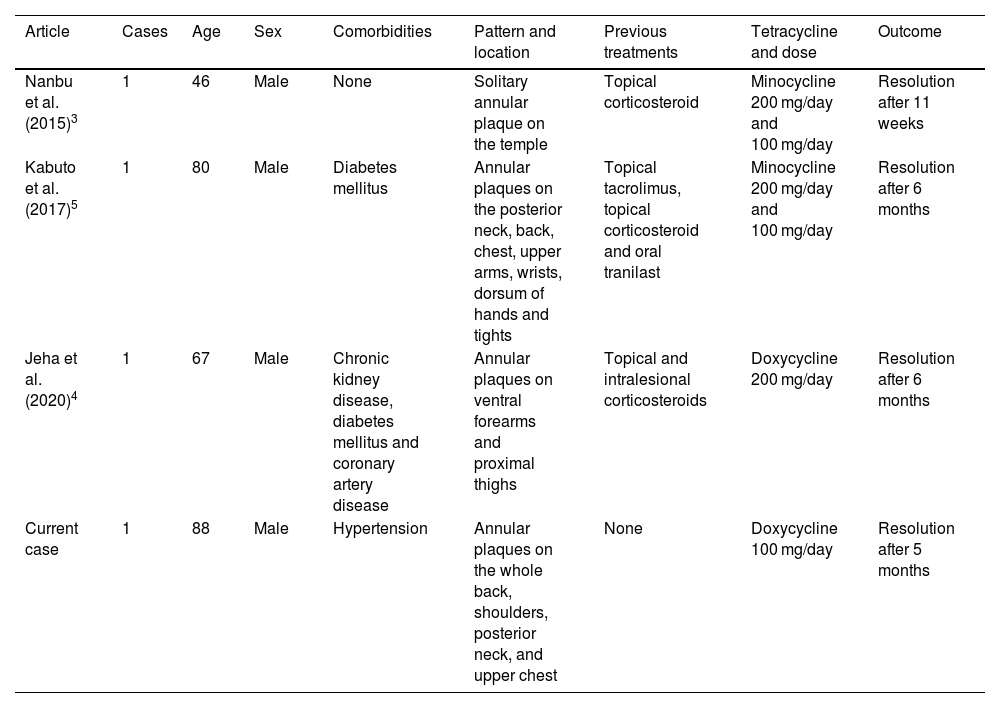
AEGCG was first described as actinic granuloma by O’Brien in 1975 to indicate the causal role of actinic damage triggering elastolysis and elastophagocytosis. However, photoaged skin with degenerative elastin changes is rarely associated with elastophagocytosis. Lesions of AEGCG are often located on nonexposed skin so other factors aside from heat and ultraviolet radiation should be considered. Several events may damage the elastic fibers and trigger the inflammatory response that leads to its phagocytosis. One of these triggers may be hyperglycemia in diabetes mellitus, as it has been frequently reported as a concomitant disease. Many other associations such as malignancies and inflammatory diseases have been described but probably the most common presentation is idiopathic.1 Despite its benign course, AEGCG can take up to several years to resolve, lesions are usually extensive and may require different treatment modalities to prevent its progression. Anti-inflammatory and anti-granulomatous effects of tetracyclines are well known but they are not regarded as a convenient treatment due to their phototoxicity and the seldom reported risk to trigger AEGCG.2 Nevertheless, tetracyclines have shown excellent outcomes with complete responses in both limited3,4 and generalized5 forms involving sun-exposed and nonexposed skin with no side effects. Table 13–5 summarizes the main features of our patient and the three previously published cases of AEGCG treated with tetracyclines.
Overview of published cases of AEGCG treated with tetracyclines
| Article | Cases | Age | Sex | Comorbidities | Pattern and location | Previous treatments | Tetracycline and dose | Outcome |
|---|---|---|---|---|---|---|---|---|
| Nanbu et al. (2015)3 | 1 | 46 | Male | None | Solitary annular plaque on the temple | Topical corticosteroid | Minocycline 200 mg/day and 100 mg/day | Resolution after 11 weeks |
| Kabuto et al. (2017)5 | 1 | 80 | Male | Diabetes mellitus | Annular plaques on the posterior neck, back, chest, upper arms, wrists, dorsum of hands and tights | Topical tacrolimus, topical corticosteroid and oral tranilast | Minocycline 200 mg/day and 100 mg/day | Resolution after 6 months |
| Jeha et al. (2020)4 | 1 | 67 | Male | Chronic kidney disease, diabetes mellitus and coronary artery disease | Annular plaques on ventral forearms and proximal thighs | Topical and intralesional corticosteroids | Doxycycline 200 mg/day | Resolution after 6 months |
| Current case | 1 | 88 | Male | Hypertension | Annular plaques on the whole back, shoulders, posterior neck, and upper chest | None | Doxycycline 100 mg/day | Resolution after 5 months |
In conclusion, tetracyclines should be considered a safe first-line treatment for patients with extensive or generalized AEGCG or a second-line option for localized forms that do not respond to conventional topical treatments.
Financial supportNone declared.
Authors' contributionsMarín-Piñero D: Approval of the final version of the manuscript; design and planning of the study; drafting and editing of the manuscript; collection, analysis, and interpretation of data; effective participation in research orientation; intellectual participation in the propaedeutic and/or therapeutic conduct of the studied cases; critical review of the literature; critical review of the manuscript.
Sola-Casas MA: Approval of the final version of the manuscript; design and planning of the study; drafting and editing of the manuscript; effective participation in research orientation; intellectual participation in the propaedeutic and/or therapeutic conduct of the studied cases; critical review of the literature; critical review of the manuscript
Perez-Muñoz N: Approval of the final version of the manuscript; design and planning of the study; drafting and editing of the manuscript; effective participation in research orientation; intellectual participation in the propaedeutic and/or therapeutic conduct of the studied cases; critical review of the literature; critical review of the manuscript
Conflicts of interestNone declared.
Study conducted at the Hospital Universitari Sagrat Cor, Barcelona, Spain.
