

Micrographic surgery was developed in the 1930s by Dr. Friedrich Mohs, using the in vivo tissue fixation method. In 1970, Stegman and Tromovitch published a series of cases using ex vivo fixation. In 1995, the Munich method was described.
Since then, surgeons have been constantly learning these techniques.1–4
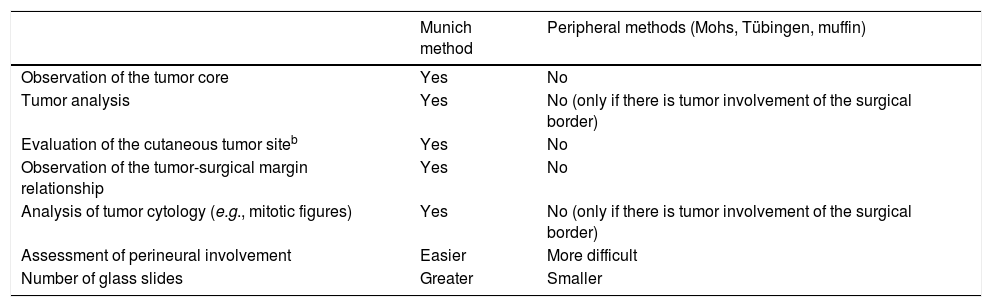
In the study by Portela et al.5 a new form of debulking assessment was described, but it is identical to the Munich method previously described in the literature. The concepts of margin and surgical border are imprecise. The authors illustrate an essential feature of the Munich method: the possibility of assessing the tumor–surgical margin relationship and observation of the tumor. Thus, it is possible to better demonstrate the subtype, cytological aspects, and tumor architecture, which have clinical and oncological relevance and are important for decision making. These factors gain importance in tumors with rarer histology and with greater metastatic potential; it also facilitates the identification of perineural invasion. In turn, peripheral methods evaluate only the surgical border, and do not observe the tumoral core. Although bread-loafing of the paraffin block is performed during debulking, the sample is smaller and the results are not available in the trans-operative period, given the time required for paraffin embedding and processing. A drawback of the fresh method is the greater chance of technical artifacts (Table 1).
Comparison between some characteristics of the Munich method and peripheral methodsa
| Munich method | Peripheral methods (Mohs, Tübingen, muffin) | |
|---|---|---|
| Observation of the tumor core | Yes | No |
| Tumor analysis | Yes | No (only if there is tumor involvement of the surgical border) |
| Evaluation of the cutaneous tumor siteb | Yes | No |
| Observation of the tumor-surgical margin relationship | Yes | No |
| Analysis of tumor cytology (e.g., mitotic figures) | Yes | No (only if there is tumor involvement of the surgical border) |
| Assessment of perineural involvement | Easier | More difficult |
| Number of glass slides | Greater | Smaller |
Even if a previous biopsy of the affected area is performed, there may be a discrepancy between the data from the incisional biopsy and the posterior excision due to sampling, as pointed out by Portela et al.5
The author of this correspondence highlights the importance of broadening the discussion of the technical and laboratory details of the various forms of micrographic surgery, including the implications of each technique for the clinical and oncological data.
Financial supportNone declared.
Author's contributionsSandro Simão Corrêa Filho: Approval of the final version of the manuscript; conception and planning of the study; drafting and editing of the manuscript; critical review of the literature; critical review of the manuscript.
Conflicts of interestNone declared.
How to cite this article: Corrêa Filho SS. On the different methods of micrographic surgery and their differences in the visualization of the tumor and surgical margin, and in the contribution to clinical and oncological aspects. An Bras Dermatol. 2020;95:546–7.
Study conducted at the Private Clinic, Blumenau, SC, Brazil.
