



Dear Editor,
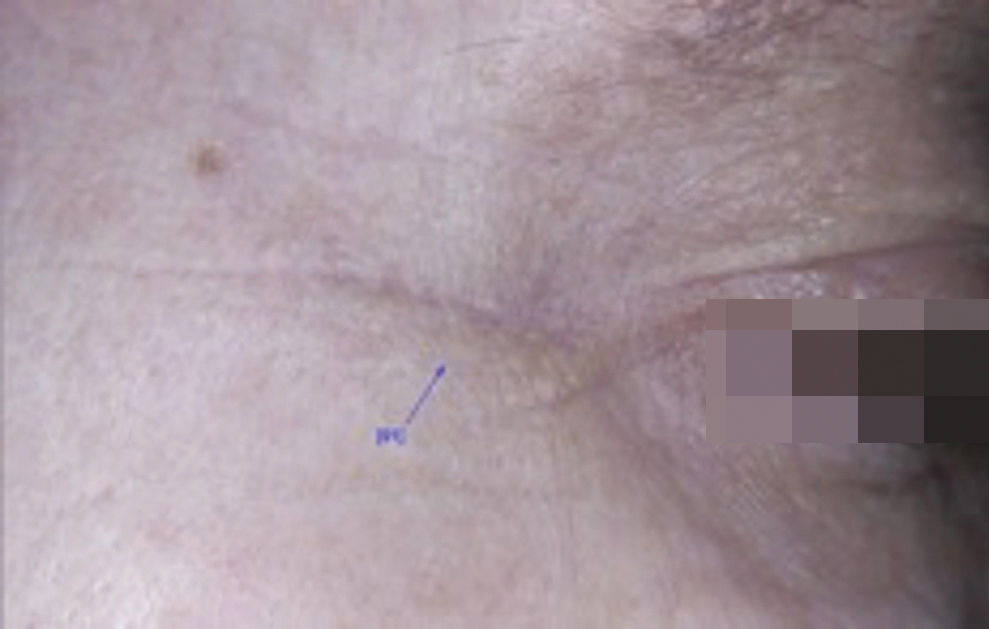
Unsightly scars can occur after tissue injury, causing psychosocial changes as well as functional impairment by altering facial expressions. Effective prevention and treatment of these scars is a challenge due to the limited understanding of the complex mechanisms involved in the healing process. There are studies demonstrating that the use of botulinum toxin A (BTXA) can reduce the intensity of tensile forces during the healing process, leading to a temporary paralysis of the muscles on the edges of the wound.1 This tensile reduction would lessen the microtrauma in the healing process and subsequently the local inflammatory response, with a lower expression of cytokines and transforming growth factorβ1 (TGF-β1) and lower fibroblast activity. These effects could result in a better and earlier maturation of the new collagen. The objective of this case series report is to evaluate the effect of the treatment with BTXA for periorbital wrinkles and for the healing after biopsies performed in the same region. In order to do that, we compared the healing after punch 6 mm biopsies performed on the ipsilateral periorbital and preauricular areas at the same time. After approval by the Committee of Ethics in Research of the Universidade Federal de São Paulo of a research project about the molecular aspects of facial wrinkles compared to skin without wrinkles and signature of the consent form, from July to August 2016, 14 women from the dermatology outpatient department were included. The participants had 2 punch 6 mm biopsies taken at the same time from the periorbital and preauricular area of the same side of the face. Immediately after suturing with mononylon 6.0, BTXA was applied only to the periorbital regions. The mean age of the participants was of 61 years (55-65 years), and they all had the Fitzpatrick (1988) phototypes III or IV. The BTXA used was abobotulinumtoxin A (Dysport®; 300 U) diluted in 1 ml saline 0.9% (ration of 1:3 compared to onabotulinum toxin). Ten units were injected into each periorbital region, with a distribution of 3 U in the upper third, 4 U in the middle third and 3 U in the lower third of the lateral orbicular muscle. One of the application points was the upper edge of the scar; the other was the lower edge. Three months later, the parameters width and visual scoring scale according to GAIS (The Global Aesthetic Improvement Scale) of the scars were assessed by the investigator, by an external observer and by the participants, comparing the scar on the periorbital region to the one on the preauricular region (Figures 1 and 2).2 Nine patients (64.3%) rated the parameters as much better; two (14.3%), as no difference; and three (21.4%), as worse. The investigator rated them as much better or better in 12 cases (85.7%), no difference in one case (7.1%) and worse in one case (7.1%). The external observer rated them as much better or better in 12 cases (85.7%) and worse in two cases (14.3%). Some scars were imperceptible (Figure 3). We performed a random dermoscopic evaluation of the scars of five patients with the deviceFotoFinder® 2007 (FotoFinder, Germany), using x 20 magnifications and carbopol gel for contact. In the scars treated with BTXA, we observed less vascular ectasia and no difference in pigmentation. Recently, a study demonstrated that the flaccid paralysis of the striated muscle for 2 to 6 months can improve hypertrophic scars.3 It is known that both in keloids and hypertrophic scars there is an increase in TGF-β1, which is responsible for regulating the proliferation of fibroblasts and the collagen synthesis, besides promoting the differentiation of fibroblasts into myofibroblasts, which in turn have an important role in the contraction and remodeling of the wound. Some studies have demonstrated that BTXA can inhibit the expression of the connective tissue growth factor (CTGF) and TGF-β1 and therefore block the proliferation of fibroblasts, that would mostly remain in the G0/G1 phase of the cell cycle.3,4 We observed that none of the participants developed a keloid or hypertrophic scar on the biopsy site (only one had past history of hypertrophic scarring in a previous surgery). In this study, the aspect of the scar on the area treated with BTXA was better than in the non-treated area. This observation confirms those of authors who believe that the toxin is not only a neurotoxin, but a multifunctional toxin that participates in the regulation of multiple genes.5 More prospective, controlled or comparative blind studies should be conducted to confirm if BTXA can represent a method preventive of unsightly scars.



Financial support: None.
Conflict of Interests: None.
